Article by Nels Ewoldsen DDS, MSD Conservative Dental Solutions Waveland, IN (private practice).
Dental caries is a “biofilm-mediated, sugar-driven, multifactorial, dynamic disease resulting in the phasic demineralization and remineralization of dental hard tissues.1 Dental caries affects most people at some point during life.2 A balanced oral environment counters ongoing demineralization cycles with equal or greater remineralization. Destabilization of the oral environment occurs when acids, endogenous and/or exogenous, remain in contact with tooth surfaces. Saliva helps neutralize acids, lubricates the oral environment and serves as a reservoir for remineralizing ions. Saliva helps maintain healthy oral biofilm. In the absence of saliva the carious process accelerates. Demineralization coupled with ineffective remineralization results in tooth surface cavitation. Cavitated teeth hold acid-producing bacteria and food debris limiting the effectiveness of biofilm control measures.3
In my practice I’ve observed two common themes regarding caries:
- patients presenting with a cavitated carious lesion frequently have additional caries affected teeth.
- patients presenting with multiple cavitated carious lesions, advanced caries, are those with the fewest resources to manage their disease.
 As with every disease intervention, good outcomes are the result of risk factor assessment and evidence-based measures to restore health. With limited resources and advancing disease, expedient and affordable interventions are of utmost importance. Although the surgical/restorative caries treatment approach seemed logical, failures has been well documented. Surgical excision of damaged dental hard tissues eradicated cesspools of infection temporarily improving oral biofilms while other disease factors remained unchecked. Today’s care standard includes caries risk assessment and risk modification/elimination resulting in less invasive, lower-cost, tooth-preserving treatments. In the case of advanced or advancing caries, however, what expedient, low-cost interventions are most practical?.
As with every disease intervention, good outcomes are the result of risk factor assessment and evidence-based measures to restore health. With limited resources and advancing disease, expedient and affordable interventions are of utmost importance. Although the surgical/restorative caries treatment approach seemed logical, failures has been well documented. Surgical excision of damaged dental hard tissues eradicated cesspools of infection temporarily improving oral biofilms while other disease factors remained unchecked. Today’s care standard includes caries risk assessment and risk modification/elimination resulting in less invasive, lower-cost, tooth-preserving treatments. In the case of advanced or advancing caries, however, what expedient, low-cost interventions are most practical?.
This article presents caries caries stabilization materials and techniques emphasizing effective affordable and expeditious interventions easily integrated into fee-for-service practice as well as community health and outreach clinics. From defining caries stabilization to technical steps, material handling tips, delegation, coding and pricing of services will be presented.
Stabilization, the process of making something more secure, less likely to fail or decline, applies to caries interventions. Both restorative and non-restorative approaches to caries stabilization have demonstrated effectiveness. Protective restorations (D2940), Interim Therapeutic Restorations (D2941), topical applications of therapeutic carioinhibitive and remineralizing agents (D1354) all offer today’s dental teams excellent caries stabilization options. Patients with advanced or advancing caries in my practice are encouraged to receive caries stabilization treatment at the diagnostic appointment. While delegation of duties and practice scope vary state-to-state, the following caries stabilization techniques are routine in my rural Indiana private practice.
Permanent Versus Deciduous Teeth with Service Life Considerations for Caries
Stabilization Restorations
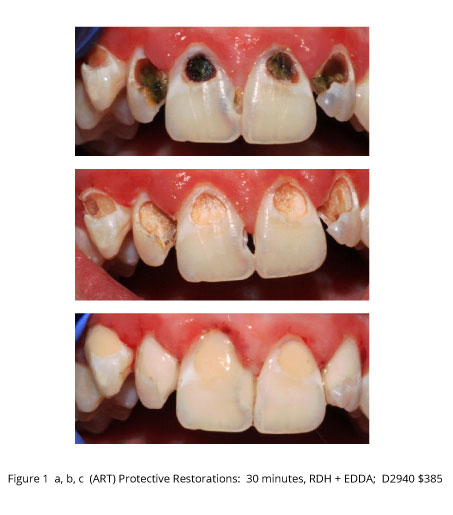
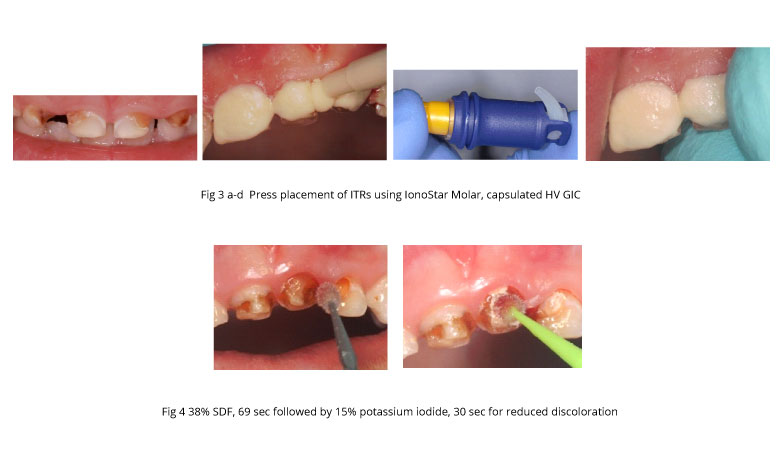
Patients presenting with advanced caries frequently cite dentophobia and financial constraints as their primary reason for not seeking care sooner. While pain is sometimes the primary motivating factor, more commonly the chief complaint is ‘I want to be able to smile’. Using Atraumatic Restorative Treatment techniques, selective excavation quickly debrides lesions without the need for local anesthetic or rotary intsrumentation, Fig 1. In Indiana dental debridement falls within the scope of dental hygiene. Glass ionomer (GI) restoration placement is then completed by an expanded function dental assistant in the dental hygiene operatory, Fig 2. Single appointment lesion debridement and tooth restoration have been shown to stabilize the oral environment reducing cariogenic bacteria and protecting the pulp.4-8 Although the value of those benefits are discussed in detail during treatment, what the patient sees is an improved smile. The expeditious placement of relatively inexpensive protective restorations stabilizes caries and gives patients confidence that their teeth are not hopeless, Fig 3,4.
{kind=link}
{kind=link}
{kind=link}
In addition to dietary modification, stepped up home care with antimicrobial and remineralizing agents, follow up protocol for protective restorations includes reevaluation of caries activity and confirmation of pulp health with planned definitive restoration placement within 6 months. This offers the patient time to prepare financially for future restorative needs. When protective restorations are surviving well at 6 months the time course for receiving definitive care may be extended. For this reason it’s important to use GI restoratives indicated for long-term use. Highly viscous GIs offer superior handling with excellent clinical durability. Also, it is common practice to prepare and place as many protective protective restorations as possible during a single visit. IonoStar Molar (Voco) is a highly viscous GI with excellent handling and physical properties. The volume of restorative GI in all of Voco’s GI capsules is nearly twice that of other HVGIs at comparable cost.
Code D2940, protective restoration applies to both deciduous and permanent teeth. Code D2941, Interim Therapeutic Restoration (ITR) applies only to deciduous teeth. The American Academy of Pediatric Dentistry policy statement cites ITRs as provisional restorations suited for young uncooperative or special needs patients or when traditional cavity preparation and tooth restoration are not possible or need to be postponed.6 Both protective restorations and ITRs reduce cariogenic bacteria levels and both preserve pulp health. In my practice, however, ITR coded restorations are generally placed in teeth of very young patients referred for specialty care, Fig 5, 6. Highly viscous, visible light cured, resin-modified GIs (HV VLC R-MGI) offer the clinical advantages of faster setting time, reduced moisture sensitivity, and improved early adhesion to tooth structure. Although rotary instrumentation is required for contouring HV VLC R-MGIs after light curing, ITRs are routinely placed without local anesthetic using IonoLux (Voco).
{kind=link}
Non-Invasive, Non-Restorative Caries Stabilization (Interim Caries Arresting Medicament Application, D1354, per Tooth) Materials and Techniques
Application of silver ion solution directly to cavitated caries lesions and/or fluoride varnish applications onto precavitated tooth surfaces, with or without antimicrobial agents effectively stabilize caries. Antimicrobial agents include ionized silver, povidone iodine and chlorhexidine. Some studies point to a synergistic effect when antibacterial agents are topically applied prior to 5% sodium fluoride varnish.
Howe’s solution (25% silver nitrate) has a long history of use in caries stabilization.7-10 There is renewed interest in silver nitrate stabilization of caries immediately prior to application of fluoride varnish.14, 15 The documented antibacterial properties of 25% silver nitrate solution applied directly to cavitated caries lesions enhance the remineralizing properties of fluoride varnish. Applying silver nitrate using a microbrush, for approximately 30 seconds followed by an application of fluoride varnish directly onto the silver nitrate treated lesion 98% non-progression of treated lesions 4 years, Fig 7,8.13
A single step caries stabilization technique using 38% silver diamine fluoride (SDF) solution (Advantage Arrest, Elevate Oral Care) has recently gained popularity in the U.S. While little consensus exists regarding SDF application time, my preference is to apply SDF using a microbrush keeping the isolated caries lesion wet with SDF for 1 minute. It is my further preference to then apply a 10-15% solution of potassium iodide directly to the SDF treated lesion minimizing initial discoloration associated with uptake of the silver ion, Fig 9,10. Non-progression of SDF treated lesions is not as high as those treated with silver nitrate plus sodium fluoride varnish Research supports reapplication of SDF to previously treated lesions 6 month intervals. Both silver nitrate and SDF temporarily discolor skin and oral mucosa necessitating good cotton roll tooth isolation techniques. It is my opinion that 38% SDF is less likely to result in soft tissue injury than 25% silver nitrate.
Although the documented success of silver ion solutions in stabilizing caries, most patients object to the permanent tooth discoloration caused by the silver ion. Alternative antibacterial treatments such as 10% povidone iodine or 2% chlorhexidine gluconate prior to sodium fluoride varnish application may be just as effective as SDF and silver nitrate treatments in stabilizing caries 14,15. Non-invasive caries treatments, a.k.a. interim caries arresting medicament applications, D1354 are billed per tooth with a fee slightly less than the fee for a preventive, full-mouth application of 5% sodium fluoride varnish, D1206.16
The interventions discussed in this article all reduce cariogenic bacterial levels and all have been shown to protect teeth from continued demineralization. These practical measures are easily implemented in most dental care settings including outreach clinics. In my practice these techniques effectively differentiate the care we provide from standard treatment approaches. Caries stabilization prior to definitive restorative care helps overwhelmed patients better understand and manage the very reason they delay dental visits. Caries stabilization offers patients hope, quickly and effectively reestablishing a stabilized oral environment.
1. https://www.ada.org/en/memter-center/oral-health-topics/caries-risk-assessment-and-management.
2. Who has cavities? Nearly all Americans, study finds. May 13, 2015, 12:09 AM EDT. NBC News, Maggie Fox.
3. Atraumatic Restorative Treatment: Quick Lesion Debridement. events.floridadental.org/Ewoldsen Caries C37 pdf.
4. Giacaman RA, Muñoz-Sandoval C, Neuhaus KW, Fontana M, Chałas R. Evidence-based strategies for the minimally invasive treatment of carious lesions: Review of the Literature.
Adv Clin Exp Med. 2018 Jul;27(7):1009-1016.
5. de Souza, Cefaly DF, Terada RS, Rodrigues CC, de Lima Navarro MF. Clinical evaluation of the ART technique using high density and resin-modified glass Ionomer Cements. Oral Health Prev Dent. 2003;1(3):201-7.
6. https://www.aapd.org/globalassets/media/policies guidelines/p itr.pdf
7. Klein, H.; Knutson, J.W., XIII. Effect of ammoniacal silver nitrate on caries in the first permanent molar. J. Am. Dent. Assoc. 1942, 29, 1420–1426. 17.
8. James, P.M.C.; Parfitt, G.J. A clinical note on the use of silver nitrate in the prevention of fissure caries in newly erupted first permanant molars. Br. Dent. J. 1954, 96, 35–36. 18.
9. Schultz-Haudt, S.; Taylor, R.; Brudevold, F. Silver nitrate treatment of proximal caries in primary molars. J. Dent. Child. 1956, 23, 184–186. 19.
10. Hyde, E.J. Caries-inhibiting action of three different topically-applied agents on incipient lesions in newly erupted teeth: Results after 24 months. J. Can. Dent. Assoc. 1973, 39, 189–193.
11. Miller, J.; Hobson, P. Silver nitrate and sodium fluoride on enamel caries. Br. Dent. J. 1959, 106, 246–249. 20.
12. Gao S, Zhao, I, Duffin S, Duangthip D, Lo E, Chu C. Revitalising Silver Nitrate for Caries Management. Int. J. Environ. Res. Public Health 2018, 15, 80
13. Duffin S. Back to the future: The medical management of caries introduction. J. Calif. Dent. Assoc. 2012;40:852–858.
14. Gostmeyer G, Schulze F, Paris S, Schwendicke F. Arrest of Root Caries Lesions via Sodium Fluoride, Chlorhexidine and Silver Diamine Fluoride In Vitro. Materials 2018,11(1), 9.
15. Milgrom PM, Tut OK, Manci LA. Topidal iodine and fluoride varnish effectiveness in the primary dentition: a quasi-experimental study. J Dent Child (Chic) 2011 Sept-Dec; 78(3): 143-7.
16. D1354 ADA Guide – Version 1 – July 17, 2017 – Page 1 of 4 ©2017 American Dental Association (ADA).